
Dr. Sisti Publishes Paper (his 100th!) on Treating Acoustic Neuromas with Radiosurgery
Dr. Michael B. Sisti, Co-Director of the Center for Radiosurgery, has had a new paper accepted for publication in the journal Neurosurgical Review. In the paper, Dr. Sisti and colleagues present research to help doctors and patients make decisions about the non-invasive treatment known as stereotactic radiosurgery for a type of tumor called acoustic neuroma.
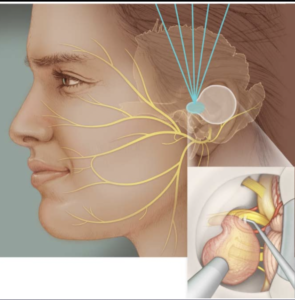
An acoustic neuroma, also known as a vestibular schwannoma, is a tumor that grows on the nerve leading from the inner ear to the brain. Vestibular schwannomas are typically slow-growing tumors, and they do not spread to other parts of the body. However, as they are located among nerves and sensitive structures of the brain and inner ear, they can adversely affect an individual’s hearing and balance. If they grow large enough, they can dangerously increase pressure in the brain.
Operating to remove the acoustic neuroma may also damage those sensitive structures. Risks of surgery can include effects on vestibular and auditory function, or on movement and sensation in the face. In deciding between treatment and watchful waiting, providers and patients must often balance the potential risks of surgery against the potential risks of continued tumor growth.
In fact, Dr. Sisti and the other authors say that treatment decisions for vestibular schwannoma can be so complex that the management of small- to medium-size tumors (< 3 cm) “remains controversial despite the significant volume of literature analyzing outcomes.”
Dr. Sisti specializes in helping patients reach a decision about treating a vestibular schwannoma. He has a wealth of experience customizing a surgical approach for each patient who is treated with surgery, and also in treating patients with radiosurgery instead of—or in combination with—traditional surgery.
Radiosurgery is a non-invasive treatment that does not require any incisions. Since it does not require the doctor to approach the tumor surgically, it has the great advantage of sparing the sensitive nearby structures. In addition, since no incisions are made, the recovery time is virtually nonexistent. Despite these advantages, the authors of this paper found that radiosurgery treatment tends to be primarily recommended at institutions that are already experienced with it.
In stereotactic radiosurgery (SRS), a stereotactic frame holds a patient’s head in position. Using 3-D computer models, doctors direct many low-level beams of radiation to converge precisely on the tumor. The goal is for the concentrated dose to disrupt the tumor’s growth, eventually shutting it down. Though the treatment itself is brief, its effect can take place over the course of months and even years.
When making a decision among options like observation, traditional surgery, and stereotactic radiosurgery, the gold standard is to rely on randomized control studies whenever possible. However, they note, “there are no randomized trials to guide management of patients with VS.”
That’s why Dr. Sisti’s new paper will be so useful to doctors and patients. The authors collect and present all the most current research, to better guide doctors everywhere in making the best-informed decisions—especially doctors who happen to be less familiar with radiosurgery.
The paper is titled “Stereotactic Radiosurgery for Management of Vestibular Schwannoma: A Short Review.” In it, Dr. Sisti and colleagues Dr. Elizabeth J. Buss, a resident in the department of radiation oncology and Dr. Tony J. C. Wang, Co-Director of Center for Radiosurgery, review the most current literature available on stereotactic radiosurgery as a treatment for vestibular schwannoma.
The doctors find that in appropriately selected patients with small to medium-size tumors, stereotactic radiosurgery performs equally as well as traditional surgery to reduce tumor size. The overall outcome is better in some instances with SRS, since it better spares the sensitive nearby structures.
Patients with tumors too large to manage with SRS alone may be treated with a combination of surgery and SRS that spares the facial nerve. This option “can provide excellent facial nerve preservation rates,” say the doctors. And patients with small tumors who opt for SRS rather than observation are less likely to need invasive surgery in the future.
The authors are pleased that this paper’s publication in a respected journal ensures that many neurosurgeons will see it. Their hope is that providers who have so far had less experience with SRS will become more familiar with the best guidelines and indications for this useful treatment option.